
Translation of the study from the Department of Biomedical Sciences at the New York Institute of Technology
Aaron Miller, Mac Josh Reandelar, Kimberly Fasciglione, Violeta Roumenova, Yan Li, and Gonzalo H. Otazu *
Department of Biomedical Sciences, NYIT College of Osteopathic Medicine, New York Institute of Technology, Old Westbury, New York, USA.
ABSTRACT
COVID-19 has spread to most countries in the world. Enigmatically, the impact of the disease differs from nation to nation. These differences are attributed to heterogeneous cultural norms, mitigation efforts, and health infrastructure. Here we propose that the differences in COVID-19 and its impact in each country could be partly explained by different national policies regarding childhood vaccination with the Bacillus Calmette-Guérin (BCG). BCG vaccination offers broad protection against respiratory infections. We compared a number of countries with BCG vaccination policies with COVID-19 morbidity and mortality. We found that countries lacking universal BCG vaccination policies (Italy, the Netherlands, and the USA) have been more severely affected compared to countries with long-standing, universal BCG policies. Countries that implemented universal BCG vaccination policies late (Iran, 1984) experienced high mortality rates, consistent with the idea that BCG protects the immunized elderly population. The BCG vaccine was also found to reduce the number of reported COVID-19 cases per country.
INTRODUCTION
The COVID-19 pandemic originated in China and has spread rapidly across all continents, affecting almost every country in the world. However, there are some striking differences in how this virus behaves from country to country. For example, Italy has implemented strict social distancing measures, yet COVID-19 mortality remains high. Conversely, Japan has had several cases, but mortality is low despite not having adopted any of the established social distancing measures. These puzzling differences have been attributed to cultural differences, as well as differences in healthcare standards and practices. Here, an alternative explanation is proposed: the country-to-country disparity in COVID-19 morbidity and mortality may be partly explained by national policies regarding the Bacillus Calmette-Guérin (BCG) vaccine.
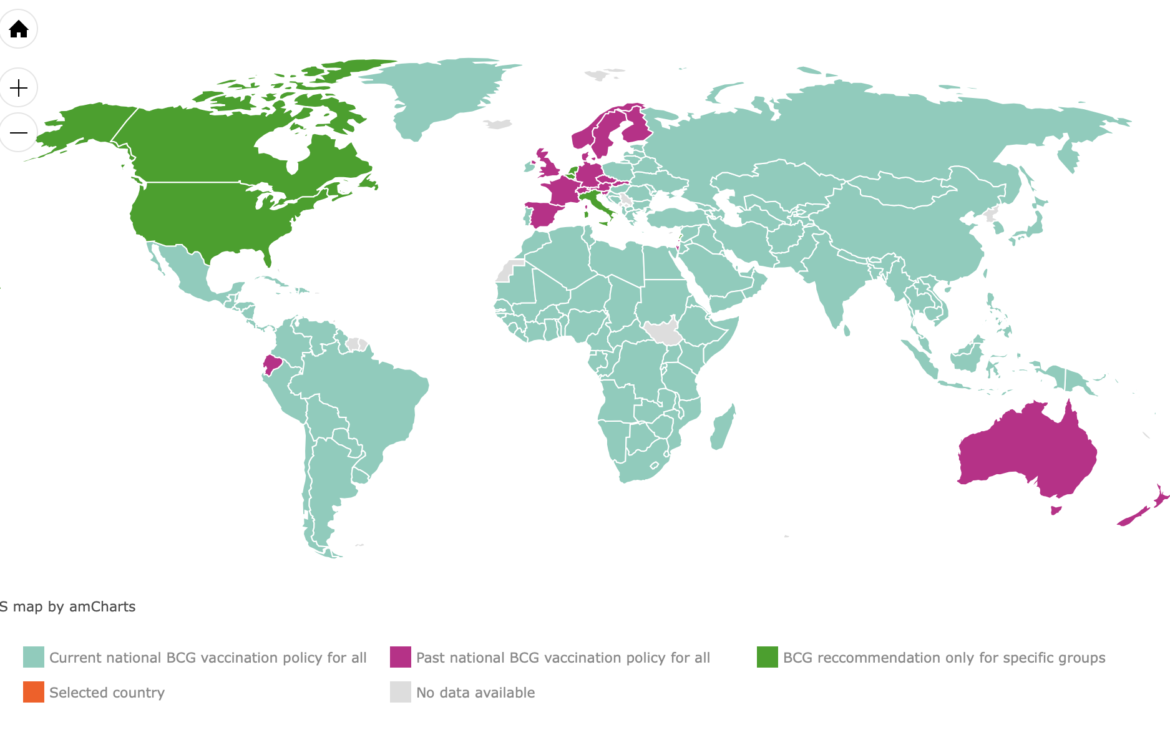
BCG is a live, attenuated strain derived from an isolate of Mycobacterium bovis. It is widely used worldwide as a vaccine against tuberculosis (TB) in many nations, including Japan and China, which have universal BCG vaccination policies for newborns. Other countries, such as Spain, France, and Switzerland, have discontinued their universal vaccination programs due to the comparatively low risk of developing M. bovis infections, as well as the variable efficacy demonstrated in preventing TB in adults. Countries such as the United States, Italy, and the Netherlands have not yet adopted universal vaccination policies for similar reasons.
Several vaccines, including BCG, have been shown to produce positive non-specific immune effects that have led to an improved response against other non-mycobacterial pathogens. For example, BCG-vaccinated mice infected with the virus showed increased production of IFN-γ from CD4 cells.
This phenomenon, termed "trained immunity," is thought to be caused by metabolic and epigenetic changes that promote genetic regions encoding pro-inflammatory cytokines. BCG vaccination significantly increases the secretion of pro-inflammatory cytokines, specifically IL-1β, which has been shown to play a vital role in antiviral immunity. Furthermore, a study conducted in Guinea-Bissau observed that children vaccinated with BCG had a 50% reduction in overall mortality, attributed to the vaccine's effect in reducing respiratory infections and sepsis. Given the current understanding of the non-specific immunotherapeutic mechanisms of the BCG vaccine and through analysis of current epidemiological data, this research aims to identify a potential correlation between the existence of universal BCG vaccination policies and morbidity and mortality associated with COVID-19 infections worldwide.
METHOD
BCG vaccination policies for all countries were compiled using the BCG World Atlas, available online at http://www.bcgatlas.org/. The database was completed with information on the dates BCG vaccination began. The data, which can be found in the appendix https://google.com/covid19-map/ , were analyzed up to the morning of March 21, 2020, and structured using Matlab scripts.
RESULTS
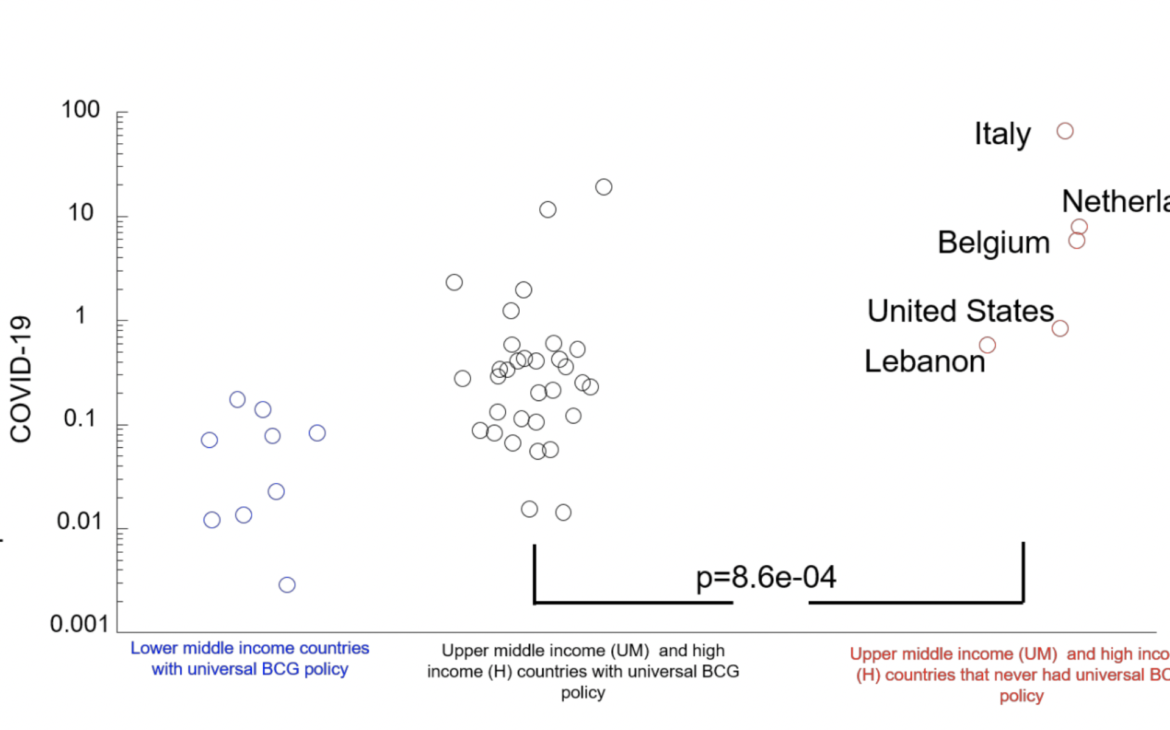
Initially, countries that had never had a universal BCG vaccination policy in place (Italy, the United States, Lebanon, the Netherlands, and Belgium) were compared to countries that currently have a universal BCG vaccination policy. Only countries with more than 1 million inhabitants were included. The mortality rate could be influenced by multiple factors, including the quality of healthcare in each country. To account for this, countries were ranked according to their 2018 GDP per capita using World Bank data: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
Countries were divided into three categories: low-income (L) countries with an annual income of $1,025 or less, lower-middle-income countries with incomes between $1,026 and $3,995, and upper-middle-income and high-income countries, which included countries with annual incomes above $3,996. To determine whether BCG vaccination was protective against COVID-19 infections, the number of deaths per million population attributed to COVID-19 was used. Most low-income countries reported zero deaths attributed to COVID-19 and have universal BCG vaccination policies in place. However, this could be due to underreporting, and these countries have been excluded from the analysis. Middle- and high-income countries with a current universal BCG vaccination policy (55 countries) had between 0.78 and 0.40 deaths per million people ( see Figure 1). In contrast, middle- and high-income countries that have never had a universal BCG vaccination policy (5 countries) had a higher mortality rate, with between 16.39 and 7.33 deaths per million people. This difference between countries was highly significant.
Middle- and high-income countries with universal BCG vaccination policies have experienced some variability in mortality rates, which increase with age. The question is whether countries that implemented universal BCG vaccination policies early would have a reduced mortality rate, as older people, who are more severely affected by COVID-19, would be protected.
Data from 28 countries with long-standing BCG vaccination policies were analyzed. There was a significant positive correlation (-0.44, p-0.02, linear correlation) between the year of establishment of universal BCG vaccination and the mortality rate, consistent with the idea that the earlier a policy was established, the greater the proportion of the elderly population would be protected. (See Figure 2)
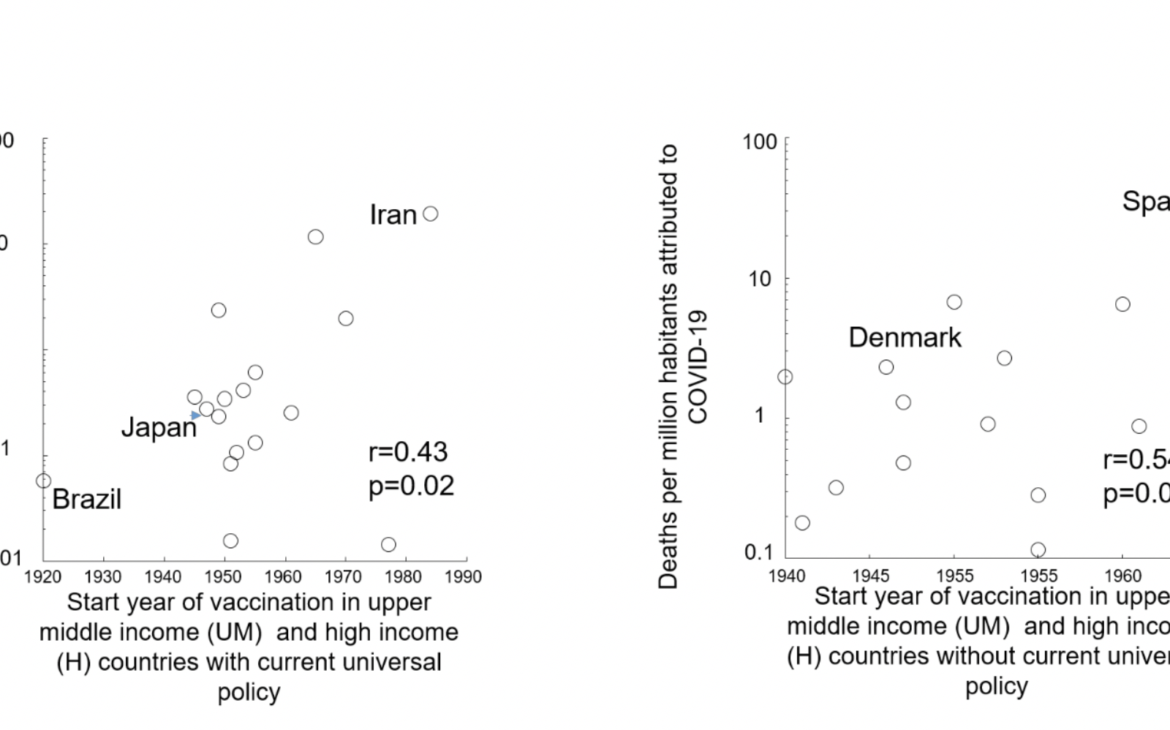
For example, Iran currently has a universal BCG vaccination policy, but it only began in 1984. Consequently, it has a high mortality rate of 19.7 deaths per million inhabitants. In contrast, Japan began its universal BCG vaccination policy in 1947 and has 100 times fewer deaths per million people. Brazil began universal vaccination in 1920, and its mortality rate is also low at 0.0573 deaths per million inhabitants.
As the number of tuberculosis cases declined in the late 20th century, several middle- and high-income European countries abandoned universal BCG vaccination policies between 1963 and 2010. It has been hypothesized that, although these countries do not currently have a universal vaccination policy, they would also show a trend whereby the earlier vaccination is initiated, the larger the proportion of the elderly population it covers, and the lower the mortality rate per million people.
Seventeen countries that abandoned their universal BCG vaccination policy were analyzed. A significant positive correlation (-0.54, p-0.02, linear correlation) was also found between the year universal BCG vaccination was established and the mortality rate. For example, Spain began its universal policy in 1965 and it lasted until 1981 (16 years), resulting in a high mortality rate (29.5 deaths per million inhabitants). In contrast, Denmark began its policy in 1946 and ended it in 1986 (40 years), resulting in almost 10 times fewer deaths per million inhabitants, with 2.3 deaths.
Evidence has been found that BCG vaccination is correlated with reduced COVID-19 mortality rates. Mortality rates are a robust measure that is less dependent on COVID-19 testing levels. However, country-specific mortality rates are related to both the number of cases present in a country and the probability of death for individual cases. The question is whether BCG vaccination would also affect the spread of the disease, given that the number of reported COVID-19 cases will depend largely on the number of tests performed per country.
Low-income countries (18) reported a lower number of COVID-19 cases per million inhabitants: 0.32 to 0.09. Middle- and high-income countries with a current universal BCG vaccination policy (55 countries) had 59.54 or 23.29 cases per million inhabitants. Consistent with the role of BCG in slowing the spread of COVID-19 in middle- and high-income countries that never had a universal BCG vaccination policy (5 countries), the number of cases per million inhabitants was found to be approximately four times higher, at 264.90 versus 134.88. This difference between countries was significant, suggesting that widespread BCG vaccination, along with other measures, could slow the spread of COVID-19.
The question is whether middle- and high-income countries with current universal vaccination policies (28 countries) would show a relationship between the number of cases and the year universal vaccination began. Interestingly, there was no significant correlation between the year vaccination began and the total number of COVID-19 cases, suggesting that early vaccination of the elderly population was not a factor in reducing the number of cases.
DEBATE
Epidemiological evidence suggests that some of the differences in COVID-19 morbidity and mortality between countries may be partially explained by their respective BCG vaccination policies. Italy, where COVID-19 mortality is very high, never implemented universal BCG vaccination. Japan, on the other hand, had one of the first cases of COVID-19 but has maintained a low mortality rate despite not implementing stricter forms of social distancing. Japan has been implementing BCG vaccination since 1947. Iran has also been severely affected by COVID-19 and began its universal BCG vaccination policy in 1984, which has left anyone over 36 years of age unprotected.
Why did COVID-19 spread in China despite its universal BCG vaccination policy since the 1950s? During the Cultural Revolution (1966–1976), tuberculosis prevention and treatment agencies were dismantled and weakened. We speculate that this may have created a pool of potential hosts who would be infected and, consequently, spread COVID-19. Currently, however, the situation in China appears to be improving.
Data suggests that BCG vaccination appears to significantly reduce COVID-19-related mortality. It also appears that the earlier a country establishes a BCG vaccination policy, the greater the reduction in its number of deaths per million inhabitants, supporting the idea that protecting the elderly population could be crucial for reducing mortality. However, there is still no evidence that late BCG inoculation boosts immunity in older adults, although it does appear to have effects in experiments with guinea pigs against Mycobacterium tuberculosis.
BCG vaccination has been shown to provide broad protection against viral infections and sepsis, raising the possibility that the protective effect of this vaccine is not only directly related to COVID-19 itself, but also against subsequent associated infections. The BCG vaccine was found to be correlated with a reduction in the number of reported COVID-19 infections. Widespread use of the BCG vaccine within a population could reduce the number of carriers and, combined with other measures, could help to slow or halt the spread of COVID-19.
Several countries use different BCG vaccination schedules and different strains of the bacteria. Data have not been broken down by strain to determine which strains are best at stopping the spread of infection and reducing mortality in the elderly population. Since each country used the same strain for its entire population, the differences between strains for different purposes should be investigated in randomized controlled trials with different subjects from the same population.
The United States and other countries like Italy, without a universal vaccination policy but with a high proportion of immigrants from countries that have universal BCG policies and use different strains, could offer the possibility of conducting epidemiological studies to determine vaccination schedules and strains that would optimize protection against COVID-19.
The correlation between the start of universal BCG vaccination and protection against COVID-19 suggests that BCG could confer lasting protection against the current strain of coronavirus. However, randomized controlled trials with BCG are needed to determine how quickly an immune response develops that protects against COVID-19. BCG is generally harmless, with the main side effect being inflammation at the injection site. However, BCG is contraindicated in immunocompromised individuals and pregnant women, so caution should be exercised when implementing these potential interventions to combat COVID-19.
REFERENCES
1.WHO | Tuberculosis. Available at: https://www.who.int/immunization/diseases/tuberculosis/en/ . (Accessed: 23rd March 2020)
2. Mathurin, KS, Martens, GW, Kornfeld, H. & Welsh, RM CD4 T-Cell-Mediated Heterologous Immunity between Mycobacteria and Poxviruses. J. Virol. 83, 3528–3539 (2009).
3. Netea, MG et al. Trained immunity: A program of innate immune memory in health and disease. Science (80-. ). 352, aaf1098–aaf1098 (2016).
4. Kleinnijenhuis, J. et al. Long-lasting effects of bcg vaccination on both heterologous th1/th17 responses and innate trained immunity. J. Innate Immun. 6, 152–158 (2014).
5. Kristensen, I., Aaby, P. & Jensen, H. Routine vaccinations and child survival: Follow up study in Guinea-Bissau, West Africa. Br. Med. J. 321, 1435–1439 (2000).
6. Zwerling, A. et al. The BCG world atlas: A database of global BCG vaccination policies and practices. PLoS Med. 8, (2011).
7. Zhou, F. et al. Articles Clinical course and risk factors for mortality of adults in patients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 6736, 1–9 (2020).
8. Japan was expecting a coronavirus explosion. Where is it? | The Japan Times. Available at: https://www.japantimes.co.jp/news/2020/03/20/national/coronavirus-explosion-expected-japan/#.XnllWahKjIU . (Accessed: 23rd March 2020)
9. Development and expectation of tuberculosis service system in China. Available at: http://www.zgflzz.cn/EN/Y2012/V34/I9/557. (Accessed: 24th March 2020)
10. Komine-Aizawa, S. et al. Influence of advanced age on Mycobacterium bovis BCG vaccination in guinea pigs aerogenically infected with Mycobacterium tuberculosis. Clin. Vaccine Immunol. 17, 1500–1506 (2010).
11. Moorlag, SJCFM, Arts, RJW, van Crevel, R. & Netea, MG Non-specific effects of BCG vaccine on viral infections. Clinical Microbiology and Infection 25, 1473–1478 (2019).
12. Horwitz, MA, Harth, G., Dillon, BJ & Masleša-Galić, S. Commonly administered BCG strains including an evolutionarily early strain and evolutionarily late strains of disparate genealogy induce comparable protective immunity against tuberculosis. Vaccine 27, 441–445 (2009).
13. Fact Sheets | Infection Control & Prevention | Fact Sheet – BCG Vaccine | TB | CDC. Available at: https://www.cdc.gov/tb/publications/factsheets/prevention/bcg.htm . (Accessed: 23rd March 2020)