Dr. Paul E. Sax
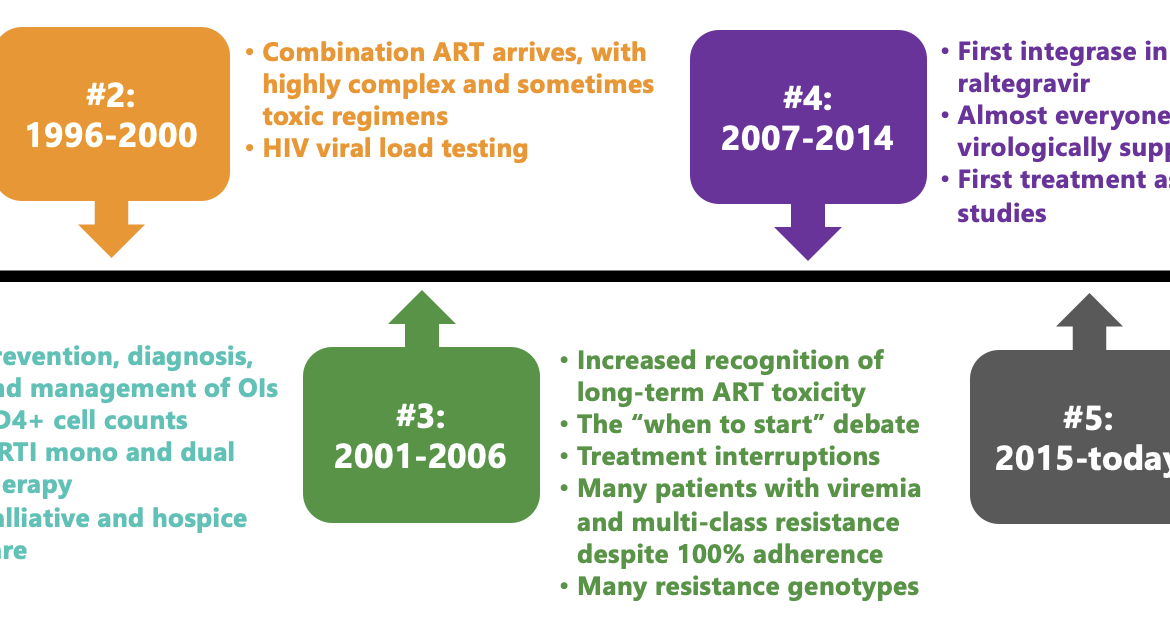
Here is a figure I made for an upcoming talk, titled "The Future of HIV Care." It summarizes several eras in HIV treatment and ends with the current unprecedented success phase in which most people with HIV take one or two pills a day, have viral suppression, and no clinically apparent immunodeficiency. HIV is often the least of their medical problems.
To put this in context, a patient at our hospital recently discovered that the cause of his several months of fatigue and weight loss was HIV and expressed relief that it wasn't diabetes or cancer. Upon hearing this, everyone on our HIV treatment team agreed that management would be easier and more likely to be successful.
I do not intend to downplay the potential severity of HIV, which, of course, can still be fatal if left undiagnosed and untreated. Too many people in this country with HIV have not been diagnosed, or have been diagnosed but are not receiving regular care or treatment . Getting them on therapy remains an urgent public and individual health priority.
But for those receiving care , as an example of medical progress, HIV treatment stands out as a phenomenal success.
This success raises the question, once again, of the role that immunologists should play in the treatment of people with HIV once they are on stable antiretroviral therapy. The last time I covered this topic here on this site almost a decade ago , we were at the end of the previous Era #4, and since then treatment has only improved.
To emphasize, I continue to believe that DI physicians and HIV specialists must play a leading role in managing new HIV diagnoses, managing opportunistic infections and other complications, interpreting resistance tests, and helping to guide treatment changes, especially as new options emerge. The nuances of identifying the best candidates for long-acting cabotegravir-rilpivirine have certainly added a recent reward to our expertise.
But what about the stable septuagenarian on one-pill ART whose main problems are hypertension, osteoarthritis, and, yes, type 2 diabetes? Who among us can claim to have kept up sufficiently with these non-ID-related issues to be their ideal primary provider? If you, as an ID specialist, were given the choice of attending an educational session by a brilliant speaker on "Advances in the Management of Invasive Fungal Infections" or "Advances in the Management of Type 2 Diabetes," which would you choose?
We shouldn't abandon HIV care, but we could potentially restructure it to be managed more like other medical specialties. Oncologists and rheumatologists, to name two examples, play a leading role in their respective diseases when treatments are active and follow-up is intensive. But no specialty assumes full primary care once patients are rock-solid.
Pushing against such a distribution of HIV care to generalists is the fact that the majority (more importantly, not all) of the primary care workforce has not been doing much in the way of HIV management. It is remarkably concentrated in a very small fraction of American physicians. As an example, a patient of mine was recently told by her primary care physician that she would not order her routine monitoring tests (CBC, full metabolic panel, and HIV RNA) because “only identification can do that.” This is, of course, an extreme example (and certainly not true), but the anecdote illustrates how far removed most people in primary care are from general HIV practice.
Another important perspective comes from our patients, some of whom we have followed for decades. They may not feel comfortable changing primary care providers, especially with a disease that, unfortunately, still carries a certain social stigma.
So let's do the poll again and see what you think. As always, I greatly appreciate your opinions on this topic in the comments section, and I'll select some for discussion!
Thank you.