
By Vicente Soriano
Faculty of Health Sciences & Medical Center, UNIR – International University of La Rioja
The first cases of AIDS were described in the United States in 1981. HIV, the retrovirus that causes the disease, took two years to be identified. Since then, more than 80 million people have been infected worldwide. Half of them have died.
Thanks to antiretroviral medication, which is being used to treat more than 30 million people living with HIV, the life expectancy of HIV-positive individuals is now similar to that of the general population. However, the virus cannot be eradicated from the body: the infection is lifelong . Furthermore, HIV has proven to be a difficult disease to treat in the search for a vaccine.
Success of antiretrovirals
Antiretroviral drugs suppress viral replication. With an undetectable viral load, the infection does not progress to AIDS, and the virus cannot be transmitted. This has allowed serodiscordant couples (one HIV-positive and one HIV-negative) to have healthy children .
On the other hand, taking antiretroviral drugs by uninfected individuals who engage in risky behaviors (for example, promiscuous sexual relations) drastically reduces the chances of infection. This is known as pre-exposure prophylaxis (PrEP).
This benefit explains a paradoxical effect (“compensation phenomenon”) on other sexually transmitted infections (STIs), which have increased in recent years, while HIV infections have fallen. As fear of HIV has decreased, syphilis and gonorrhea have increased . It should be noted that PrEP use is particularly widespread among the gay community.
Failure of HIV vaccines
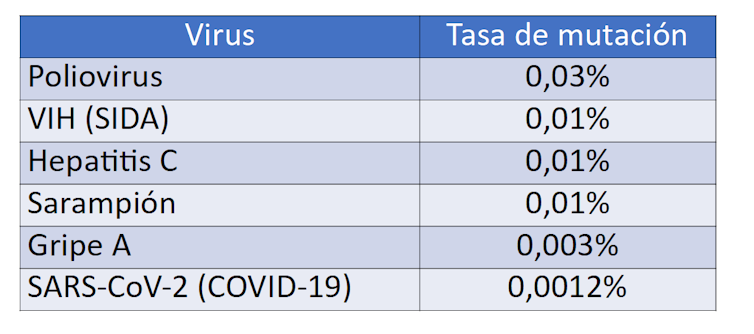
A vaccine against the AIDS virus has not been achieved largely due to the high genetic variability of the virus. The error rate of the HIV polymerase is 0.01%, meaning that each new copy of retroviral RNA has one nucleotide different from the parent copy.
In comparison, the polymerases of polio, influenza, or coronavirus viruses have much greater replication fidelity, resulting in a less diverse viral population. This antigenic stability facilitates the development of effective vaccines against COVID-19.
Because millions of viral particles are produced daily in each infected person, HIV is said to circulate as a quasispecies —that is, a dynamic constellation of genomic sequences around a master (or average) sequence. In the body, if environmental pressure includes antiretrovirals or antibodies, circulating variants of the virus that evade (resistant) the drugs or immunity are selected. Therefore, HIV causes a chronic, persistent, lifelong infection in those infected.
Vaccines and antivirals against COVID-19
The situation with SARS-CoV-2 coronavirus infection is very different. Everything has happened very quickly. From the description of the first cases of pneumonia in late 2019 in Wuhan, China, the identification of the causative virus occurred a month later. The first antiviral, remdesivir, was approved after six months, and the first vaccines began to be administered before a year had passed.
Since the start of the pandemic, 80 million people have been confirmed infected in a year, of whom 2 million have died. Almost all the others have recovered, with the virus being eliminated from the body by the immune system. In any case, the specific antibodies that indicate a past coronavirus infection are no longer detectable in 15% of patients after 6 months, especially in those who had an asymptomatic infection. This seems to explain cases of reinfection , although the symptoms are usually milder in subsequent episodes.
SARS-CoV-2 is primarily transmitted through the air, similar to the flu, by inhaling viral particles expelled by infected individuals when they sneeze and talk. The larger the viral load, the greater the risk of infection . Therefore, masks and outdoor activities are important for reducing coronavirus transmission.
Unlike HIV, the SARS-CoV-2 coronavirus exhibits little genetic variability. Its antigenicity is stable, resulting in an effective immune response. Similarly, the selection of antiviral resistance is expected to be infrequent. While combination therapy is necessary for sustained suppression of viral replication in HIV, monotherapy may be sufficient for the coronavirus. However, a potent antiviral must be identified, given that remdesivir has limited in vivo activity.
The vaccines that have begun to be administered protect against severe forms of COVID-19, but they do not appear to completely prevent infection in the upper respiratory tract, so the risk of transmission does not disappear entirely. Perhaps new generations of vaccines or the administration of multiple (booster) doses will achieve greater immunity.